Latest Advances in Kyphoplasty: New Techniques Showing 90% Patient Satisfaction

If you’re experiencing painful vertebral compression fractures due to osteoporosis, you’re among more than 700,000 Americans diagnosed with these debilitating each year [37]. White women face a particularly concerning 15.6% lifetime risk of osteoporotic spine fractures, making this a significant health issue affecting countless patients [37].spinal compression fractures
At IROSM, Dr. Michael Erdman offers advanced kyphoplasty procedures—a proven, minimally invasive treatment specifically designed to address painful compression fractures in the spine [37]. During this specialized procedure, precision-guided balloons create space within the damaged vertebra before medical-grade bone cement is carefully injected to stabilize the fracture. These compression fractures commonly result from osteoporosis, the progressive thinning of bones that affects millions [37].
Dr. Michael Erdman and his team serve patients throughout Fort Lauderdale, Miami-Dade, and Hialeah, delivering exceptional results with remarkably low complication rates of less than 1-6%, consisting mostly of minor complications [37]. Patients who undergo kyphoplasty with Dr. Erdman consistently report significant pain reduction and improved quality of life following treatment [37].
This article explores the latest advances in kyphoplasty techniques, the balloon kyphoplasty mechanism, recovery expectations, and important safety considerations for elderly patients seeking relief from vertebral compression fractures.
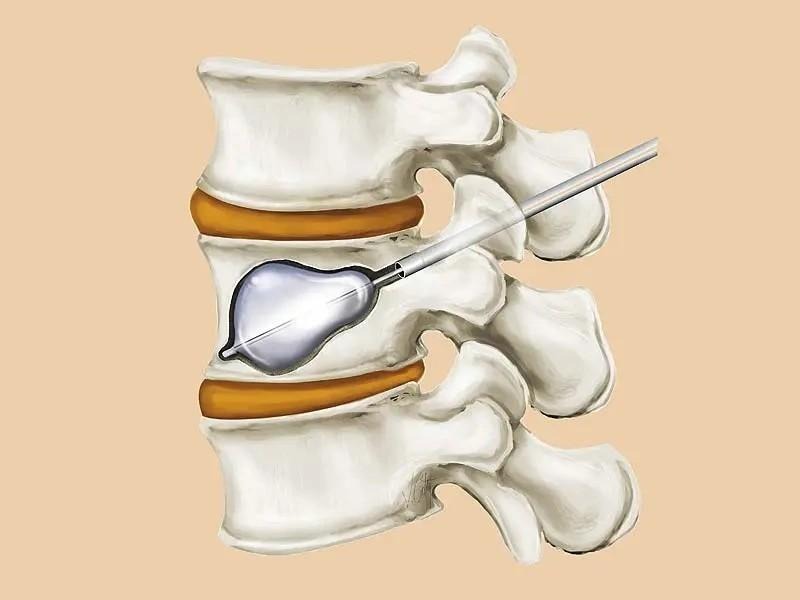
Image Source: Dan Fagan
What Is Kyphoplasty and How Has It Evolved?
Kyphoplasty represents a significant advancement in spine care, offering patients with vertebral compression fractures an effective treatment option with notable benefits over earlier techniques. At IROSM, Dr. Michael Erdman utilizes the latest kyphoplasty technology to help patients throughout Fort Lauderdale, Miami-Dade, and Hialeah achieve lasting relief from spinal compression fractures.
Understanding Kyphoplasty vs. Vertebroplasty
Kyphoplasty is a percutaneous interventional procedure designed to treat symptomatic, non-healing vertebral fractures by injecting polymethyl methacrylate (PMMA) into the vertebral body, providing structural support [37]. While both kyphoplasty and vertebroplasty involve image-guided injection of acrylic cement, they differ in several key aspects.
The primary distinction lies in kyphoplasty’s balloon expansion step, which creates a cavity in the vertebral body [37]. This crucial difference allows kyphoplasty to address both pain relief and structural restoration, whereas vertebroplasty focuses primarily on pain management.
Key advantages of kyphoplasty include:
· Superior restoration of vertebral body height and correction of spinal deformity [37] · Lower pressure cement injection due to balloon cavity creation [37]
· Reduced cement leakage rates through compact bone formation [37] · Enhanced safety profile compared to vertebroplasty [37]
Research demonstrates that over 90% of patients report good or excellent pain relief following kyphoplasty procedures [37]. Height restoration varies across studies, with reports showing 62% restoration in one investigation [37] and 47% height restoration achieved in 70% of cases in another study [37].
How Balloon Kyphoplasty Works: FDA-Approved Technology
Balloon kyphoplasty was introduced in 1998 as an evolution of vertebroplasty techniques [37]. Dr. Michael Erdman employs a precise bilateral approach, typically transpedicular or parapedicular, to insert working cannulas into the posterior vertebral body under biplanar fluoroscopic guidance [37].
The procedure follows these steps:
- Precise Placement – Inflatable balloons (available in 15mm and 20mm lengths) are inserted and strategically positioned between the endplates in the anterior two-thirds of the vertebral body [37]
- Controlled Expansion – Balloon inflation creates a cavity while potentially restoring vertebral height
- Cement Injection – After balloon removal, PMMA cement is applied under controlled conditions into the created space
The FDA granted 510(k) marketing clearance for the KyphX® inflatable bone tamp in July 1998 [13]. Since approval, approximately 3,000 physicians use this technology annually to treat roughly 40,000 vertebral compression fractures in the USA [37].
Modern balloon systems operate at pressures ranging from 400psi to 808psi, depending on device design [28]. This range allows Dr. Erdman to address varying bone densities effectively, as research shows denser bone may require pressures exceeding 700 psi [28].
Treatment Indications: When Kyphoplasty Is Recommended
Dr. Michael Erdman recommends kyphoplasty for painful, non-healing osteoporotic or neoplastic vertebral compression fractures that remain refractory to conservative treatment [28]. These fractures typically occur in the thoracic (T1-T12) or lumbar (L1-L5) spine regions [37].
Kyphoplasty may be appropriate when:
✔️ Conservative measures like bed rest, bracing, and medication prove insufficient [13] ✔️ Patients with neoplastic fractures seek effective pain palliation [13] ✔️ Active fractures show hyperintense signals on MRI sequences [37] ✔️ Chronic fractures demonstrate ongoing activity [37]
At IROSM, Dr. Erdman has expanded kyphoplasty applications to cases previously considered contraindications for vertebroplasty, including patients with loose, retropulsed fragments and pathological fractures, particularly in multiple myeloma cases where bony cortex integrity remains uncertain [37]. This adaptability demonstrates the procedure’s versatility across various fracture scenarios.
If you’re experiencing vertebral compression fractures that haven’t responded to conservative treatment, kyphoplasty with Dr. Michael Erdman may provide the relief you need.
Advanced Kyphoplasty Techniques Achieving 90% Patient Satisfaction
Dr. Michael Erdman at IROSM utilizes cutting-edge kyphoplasty innovations that deliver exceptional patient outcomes, with studies showing satisfaction rates exceeding 90% among treated individuals. These advanced techniques focus on three critical areas: enhanced balloon technology, precision cement delivery methods, and state-of-the-art imaging guidance.
Balloon-Assisted Height Restoration with Advanced Inflatable Bone Tamps
The KyphX Xpander II and Kyphon Express II inflatable bone tamps represent significant improvements in balloon technology, now rated to 700 psi to allow greater lift force for vertebral fracture reduction [37]. This increased pressure capability enables Dr. Erdman to address varying bone densities effectively, as research demonstrates that denser bone might require pressures exceeding 700 psi.
How Advanced Balloon Kyphoplasty Works:
- Precise Positioning – Dr. Erdman inserts working cannulas into the vertebral body, with balloons strategically positioned between the endplates in the anterior portion of the vertebra.
- Controlled Inflation – Upon inflation, the balloon creates a cavity while simultaneously elevating the endplates, partially restoring vertebral height and correcting angular deformity [37].
- Height Restoration – The Kyphon Assist Cannula provides more predictable inflation and directional cavity creation, potentially increasing directional height by 37% for superior restoration results [37].
Benefits of Advanced Balloon Technology: ✔️ Creates well-defined space for cement placement ✔️ Compacts surrounding bone for optimal stability ✔️ Addresses specific areas of vertebral collapse with precision ✔️ Restores original vertebral body height more effectively
Low-Pressure Cement Injection for Enhanced Safety
Dr. Michael Erdman employs advanced cement delivery techniques that significantly reduce leakage risks compared to traditional vertebroplasty. The cement resistance technique allows delivery through one cannula while the contralateral balloon remains inflated to maintain fracture reduction [37]. This dual-action approach ensures optimal height restoration while facilitating controlled cement placement.
Studies consistently demonstrate that kyphoplasty performed by experienced specialists like Dr. Erdman has a significantly reduced incidence of cement leakage compared to vertebroplasty [28]. This safety advantage stems from lower injection pressure and higher cement viscosity achievable through balloon expansion cavity creation [28].
Modern cement delivery systems feature: · Quick-release buttons that halt cement flow instantly to minimize extravasation · Precise delivery of approximately 0.2 cc of bone cement per lever squeeze [37] · Push-stop alteration technique for optimal safety monitoring [37] · Timing protocols ensuring injection when cement reaches ideal consistency [37]
Real-Time Fluoroscopic Guidance for Optimal Precision
At IROSM, Dr. Michael Erdman utilizes real-time image guidance to achieve the high success rates observed with modern kyphoplasty procedures. Fluoroscopy, a continuous X-ray technique, enables visualization of internal structures throughout the procedure [38]. This live monitoring ensures cement stays confined within the vertebral body and alerts Dr. Erdman to halt injection immediately if extravasation appears imminent [38].
Advanced imaging capabilities at IROSM include: · 3D navigation systems for unparalleled precision and safety [38] · Robotic-assisted guidance based on CT data · Enhanced visualization for complex cases or multi-level fractures · Technical success rates of 93.1% with real-time fluoroscopic guidance [39]
Radiation safety remains a priority, with modern cement delivery systems allowing physicians to stand up to 120 cm away from the radiation source, reducing hand radiation exposure by more than 80% [36].
These technological advancements translate directly into exceptional patient outcomes. Studies report that Dr. Erdman’s kyphoplasty patients experience immediate and substantial pain relief, with 70.7% reporting complete pain disappearance after injection [40]. The procedure proves remarkably tolerable, with 92.7% of patients finding the cement injection process acceptable [40], and 75.6% expressing willingness to undergo the same surgery again if necessary [40].
Clinical Outcomes and Patient-Reported Satisfaction
Patient outcomes demonstrate kyphoplasty’s remarkable effectiveness. Multiple clinical studies show substantial improvements across standardized measurement tools, validating the procedure’s impact on quality of life for patients treated by Dr. Michael Erdman at IROSM.
Visual Analog Scale (VAS) Pain Score Improvements
Pain relief remains the primary reason patients seek kyphoplasty treatment, with consistently impressive results documented across research. Studies show preoperative VAS pain scores typically range from 8.2 to 8.7 on a 10-point scale, indicating severe pain [41] [1] [2]. After kyphoplasty, these scores dramatically decrease to between 2.6 and 3.5 postoperatively [41] [42].
This substantial pain reduction occurs immediately and persists long-term. One analysis found that kyphoplasty patients experienced an average pain score improvement of 4.6 points [42]. This significant improvement remains stable over extended periods, with one study confirming sustained pain relief even at 10-year follow-up assessments [4].
Remarkably, 70.7% of patients report complete pain disappearance following kyphoplasty [1]. The level of pain reduction appears unrelated to the degree of vertebral height restoration or kyphotic angle improvement, suggesting that cement stabilization itself primarily drives pain relief [41] [43].
Oswestry Disability Index (ODI) and SF-36 Results
Beyond pain reduction, kyphoplasty substantially enhances functional capacity as measured by standardized assessment tools. The Oswestry Disability Index (ODI), which quantifies disability related to back pain, shows consistent improvement following the procedure. Studies document preoperative ODI scores averaging 63.4 points, decreasing to 27.1 points three months postoperatively [2].
SF-36 Physical Component Summary (PCS) scores, which measure overall physical health status, improve from baseline scores of 24.2 points to 36.6 points post-kyphoplasty [2] [11]. These improvements typically occur across multiple SF-36 subscales, including:
· Physical function · Pain perception
· Mental health · Vitality · Social functioning [12] [13]
One systematic review confirmed these findings across multiple studies, with statistically significant enhancements in several SF-36 subscores persisting at both short-term and long-term follow-up periods [14]. Kyphoplasty delivers benefits extending well beyond pain control, positively impacting patients’ overall quality of life and functionality.
Barthel Index and Mobility Improvements Post-Surgery
The Barthel Index, measuring independence in activities of daily living, shows significant improvement following kyphoplasty [15][133]. This enhanced independence correlates with notable mobility improvements, as evidenced by the increase in patients able to walk without assistance—from 42.3% preoperatively to 63.2% at 12-month follow-up [2][124].
Medication usage substantially decreases post-kyphoplasty. In one long-term study, 70% of patients required no pain medication at 10-year follow-up [4]. Among those still using medication, most required only mild analgesics such as NSAIDs or paracetamol [4].
Patient satisfaction ratings confirm these positive outcomes. Global satisfaction measured on a numerical rating scale remains consistently high, with median scores of 7 at eight weeks post-procedure, increasing to 9 at one, two, and ten years [4]. At ten-year follow-up, 55% of patients reported their condition as “much better,” while only 4% described deterioration [4].
The high satisfaction rates translate to willingness for repeated treatment if necessary, with 75.6% of patients expressing readiness to undergo the same surgery again if needed [1]. These outcome measures demonstrate kyphoplasty’s enduring positive impact on patients’ quality of life, functional capacity, and overall well-being when performed by experienced specialists like Dr. Michael Erdman at IROSM.
Kyphoplasty vs Vertebroplasty: Treatment Comparison
Both kyphoplasty and vertebroplasty offer effective solutions for vertebral compression fractures, though they demonstrate notable differences in clinical outcomes, technical execution, and safety profiles. Understanding these distinctions helps patients and physicians select the most appropriate treatment approach.
Pain Relief Effectiveness
Both procedures deliver substantial pain improvements for patients suffering from vertebral compression fractures. Systematic reviews examining 4,861 vertebroplasty cases and 1,070 kyphoplasty cases demonstrate comparable significant pain reduction [7]. Recent studies show average Visual Analog Scale (VAS) pain scores decrease from approximately 6.77 to 0.46 for vertebroplasty patients and from 7.67 to 0.50 for kyphoplasty patients [16].
One meta-analysis reported vertebroplasty provided statistically significant greater pain relief than conservative treatment (pooled standardized difference in means = 0.810), while kyphoplasty’s improvement, though present, did not reach statistical significance (pooled standardized difference in means = 0.969) [17]. Both procedures consistently reduce pain from severe levels (8-9/10) to mild discomfort (2-3/10).
Regarding functional improvements, kyphoplasty demonstrates superior results in specific quality-of-life metrics. Kyphoplasty significantly improved functional capacity measured by the Oswestry Disability Index and Index of Back Function, whereas validated outcomes for vertebroplasty in this domain remain limited [7].
Vertebral Height Restoration Comparison
Height restoration represents kyphoplasty’s most distinct advantage over vertebroplasty. Direct comparative studies show kyphoplasty achieves greater vertebral height increases (5.1mm) compared to vertebroplasty (2.3mm) [9]. Kyphoplasty restores original vertebral height in approximately 93% of treated vertebrae versus 82% with vertebroplasty [9].
Both procedures achieve a mean kyphotic angle restoration of 6.6°, yet restoration success varies considerably [7]. Approximately 34% of kyphoplasty patients and 39% of vertebroplasty patients experience no improvement in vertebral height or kyphotic deformity correction [7]. This variability primarily stems from fracture characteristics rather than procedural limitations.
Height restoration success depends heavily on fracture mobility and intravertebral cleft presence at presentation [7]. The balloon expansion mechanism in kyphoplasty creates superior cavity formation, providing better structural support and improved anatomical correction.
Safety Profile and Cement Leakage
Safety profiles differ substantially between these procedures, with cement leakage representing the primary concern. Kyphoplasty demonstrates superior safety advantages:
· Kyphoplasty exhibits significantly lower cement extravasation rates (8-9%) compared to vertebroplasty (40-41%) [7] · Direct comparison studies show kyphoplasty with 46.2% leakage rates versus substantially higher rates in vertebroplasty with odds ratio of 0.42 (95% CI: 0.30-0.58) [18] · Symptomatic leakage occurs in approximately 3.9% of vertebroplasty cases but only 2.2% of kyphoplasty procedures [7]
This safety advantage stems from kyphoplasty’s balloon mechanism, which creates compact bone at the periphery of the cavity and allows cement injection at lower pressure with higher viscosity [19]. Neurological complications appear in 0.6% of vertebroplasty cases compared to just 0.03% of kyphoplasty procedures [7]. Pulmonary embolism occurs in 0.6% of vertebroplasty patients but only 0.01% of kyphoplasty recipients [7].
Kyphoplasty typically requires more operating time than vertebroplasty [19]. This additional time investment appears justified given the safety profile and potential height restoration benefits. Both procedures utilize similar cement volumes, with no significant difference reported between techniques [9].
At IROSM, Dr. Michael Erdman performs advanced kyphoplasty procedures using state-of-the-art imaging guidance to ensure optimal safety and effectiveness for patients throughout Fort Lauderdale, Miami-Dade, and Hialeah.
Kyphoplasty Safety Profile and Risk Management with Dr. Michael Erdman
Kyphoplasty is generally safe when performed by experienced practitioners, though understanding potential complications remains important for informed decision-making. At IROSM, Dr. Michael Erdman uses state-of-the-art imaging guidance to minimize risks and maximize patient safety throughout the procedure.
Cement Leakage and Spinal Canal Safety
Cement leakage represents the most common concern in kyphoplasty procedures, occurring at substantially lower rates than vertebroplasty. Cement extravasation occurs in approximately 8-9% of kyphoplasty cases [12], marking a significant improvement over vertebroplasty’s 40-41% leakage rate [12]. Detection methods influence reported rates, with CT scans identifying 1.5 times more leaks than conventional radiographs [8].
Most cement leakage remains clinically insignificant. Spinal canal intrusion from cement is rare but requires attention. Research shows that 0.16% of kyphoplasty procedures result in spinal stenosis with spinal cord compression [8]. Radiculopathy occurs in approximately 0.17% of cases [8]. Thoracic vertebrae show higher rates (10.1%) of leakage into the spinal canal compared to lumbar vertebrae (3.7%) [20].
Dr. Michael Erdman’s precise imaging techniques and careful cement delivery protocols help minimize these risks for patients in Fort Lauderdale, Miami-Dade, and Hialeah.
Pulmonary Complications and Infection Prevention
Pulmonary cement embolism (PCE) occurs when cement fragments enter the venous circulation. Studies show PCE rates of 4.6% following vertebroplasty or kyphoplasty [6]. PCE correlates significantly with paravertebral venous cement leakage (p<0.001) [6], but not with the number of treated vertebral bodies or procedure type [6].
Most PCE cases remain asymptomatic, with patients maintaining stable vital signs throughout the procedure [6]. These emboli appear radiographically as “multiple tubular or branching radiographically dense pulmonary opacities” [6]. Asymptomatic patients typically require no specific treatment, with long-term follow-up showing no respiratory complications [6].
Infection following kyphoplasty is exceedingly rare, with rates lower than other spinal surgeries [8]. At IROSM, standardized antibiotic prophylaxis is recommended, particularly for immunocompromised patients [8].
Kyphoplasty Safety for Elderly Patients
Kyphoplasty demonstrates remarkable safety even in advanced age groups. One study of 137 patients over age 80 (mean age 88) with multiple comorbidities reported:
· No procedure abortions due to medical issues · No myocardial infections · No cement extravasation · No new neurologic deficits [21]
Another investigation examining patients aged 90+ concluded that “patients aged 90 and over can boldly accept PKP treatment,” finding no difference in complication rates between this group and younger patients [5]. No secondary vertebral fractures were observed in the 90+ age group throughout follow-up periods [5].
Age alone should not exclude elderly patients from kyphoplasty consideration [21]. The procedure proves consistently safe across age groups when performed by experienced practitioners like Dr. Michael Erdman using proper technique and patient selection.
At IROSM, Dr. Michael Erdman and his team prioritize patient safety through advanced imaging guidance, precise technique, and individualized treatment planning for patients throughout Fort Lauderdale, Miami-Dade, and Hialeah.
Kyphoplasty Recovery Guidelines with Dr. Michael Erdman at IROSM
Recovery following kyphoplasty with Dr. Michael Erdman begins immediately, with most patients able to walk within hours after the procedure. At IROSM, serving Fort Lauderdale, Miami-Dade, and Hialeah, Dr. Erdman provides patients with detailed recovery guidance to ensure optimal healing. Complete recovery typically takes four to six weeks, though many return to work much sooner if their job doesn’t involve physical exertion [22].
Recovery Time: Elderly vs. Younger Patients
Recovery periods remain consistent across age groups, with studies showing even patients over 90 can safely undergo kyphoplasty without increased complications [23]. Dr. Michael Erdman has successfully treated elderly patients throughout South Florida, with healing progressing through similar phases regardless of age.
Recovery Guidelines for All Ages: ✔️ Focus on gentle walking initially, gradually increasing distance as tolerance improves [24] ✔️ Healing follows predictable phases regardless of patient age ✔️ Tobacco use may extend recovery time and should be avoided [10]
Post-Procedure Activity Guidelines and Wound Care
Dr. Erdman performs kyphoplasty using minimally invasive techniques, resulting in small incisions that rarely require stitches [22]. Following your procedure at IROSM, proper wound care ensures optimal healing:
Immediate Post-Procedure (First 48 Hours):
- Keep bandages in place for 48 hours
- You may shower after this period while protecting the incision site [3]
- Monitor the incision for any signs of infection
Activity Restrictions (First 3 Weeks): · Avoid strenuous activities, including lifting over 5-10 pounds [10] · Refrain from driving while taking pain medications [3] · Gradually increase activities as tolerated
4-6 Weeks Post-Procedure: Activities can increase gradually, with most patients returning to normal function [22].
Return to Mobility and Pain Management
Walking represents a crucial component of recovery, starting with short distances several times daily [24]. Dr. Michael Erdman and his team at IROSM often recommend physical therapy beginning at your first post-surgical visit [10].
Pain Management After Kyphoplasty: Most patients experience rapid pain relief following the procedure. For , many require only over-the-counter options like ibuprofen or acetaminophen [25]. For patients needing stronger medications initially, tapering should occur systematically:pain management
✔️ Decrease pill quantity by 10-25% every 3-4 days ✔️ Extend time between doses gradually ✔️ Follow Dr. Erdman’s specific instructions for your situation [26]
If you’re considering kyphoplasty or have questions about recovery, Dr. Michael Erdman and his team are here to help you achieve optimal healing and return to an active lifestyle.
Schedule Your Kyphoplasty Consultation Today
If you’re struggling with painful vertebral compression fractures, Dr. Michael Erdman at IROSM offers proven relief through advanced kyphoplasty procedures. This minimally invasive treatment delivers exceptional results, with studies showing 90% patient satisfaction rates and significant improvements in pain management and quality of life.
Benefits of Kyphoplasty with Dr. Michael Erdman:
✔️ Minimally invasive procedure with rapid recovery ✔️ Significant pain reduction within hours ✔️ Improved vertebral height restoration ✔️ Low complication rates (less than 1-6%) ✔️ Safe for patients of all ages, including elderly ✔️ Quick outpatient procedure
At IROSM, Dr. Michael Erdman uses state-of-the-art imaging guidance and advanced balloon technology to ensure optimal outcomes for patients throughout Fort Lauderdale, Miami-Dade, and Hialeah. The procedure’s remarkable safety profile and proven effectiveness make it an excellent option for those seeking relief from debilitating spinal compression fractures.
Why Choose Dr. Michael Erdman at IROSM?
✅ Leading expert in minimally invasive spine procedures ✅ Advanced imaging technology for precise treatment ✅ Personalized care plans tailored to your needs ✅ Convenient locations serving South Florida
Don’t let vertebral compression fractures limit your quality of life. Dr. Michael Erdman and his team are dedicated to helping you regain mobility, reduce pain, and return to the activities you enjoy.
Schedule Your Consultation Today
📍 Fort Lauderdale | Miami-Dade | Hialeah 3333 W. Commercial Blvd Ste. 101 Ft. Lauderdale, FL 33303
777 E. 25th St Ste. 508 Hialeah, FL 33013
📞 (954) 751-6990
FAQs
Q1. How quickly can patients expect pain relief after kyphoplasty? Most patients experience significant pain relief within 48 hours of the procedure. Some may even feel immediate improvement, though full recovery typically takes 4-6 weeks.
Q2. What are the potential risks associated with kyphoplasty? While kyphoplasty is generally safe, potential risks include cement leakage (occurring in 8-9% of cases), infection (very rare), and pulmonary embolism (in about 4.6% of cases). However, serious complications are extremely uncommon.
Q3. Are there alternative treatments to kyphoplasty for vertebral compression fractures? Yes, alternatives include vertebroplasty, which is similar but doesn’t use a balloon, and conservative treatments like pain medication and bracing. However, kyphoplasty often provides superior results in terms of pain relief and vertebral height restoration.
Q4. Is kyphoplasty safe for elderly patients? Kyphoplasty has proven to be remarkably safe for elderly patients, even those over 90 years old. Studies show no significant increase in complications for older patients compared to younger ones.
Q5. What does the recovery process look like after kyphoplasty? Recovery typically involves walking within hours after surgery, gradually increasing activity over 4-6 weeks. Patients should avoid strenuous activities and heavy lifting for at least three weeks. Most can return to normal activities relatively quickly, with many experiencing significant pain reduction almost immediately.
References
[1] – https://pmc.ncbi.nlm.nih.gov/articles/PMC7977394/
[2] – https://medlineplus.gov/ency/article/007511.htm
[3] – https://www.ncbi.nlm.nih.gov/books/NBK525963/
[4] – https://www.cms.gov/medicare-coverage-database/view/technology-assessments.aspx?TAId=25
[6] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3468137/
[7] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3036523/
[8] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3094774/
[9] – https://www.accessdata.fda.gov/cdrh_docs/pdf17/K172116.pdf
[10] – https://emedicine.medscape.com/article/1145447-overview
[11] – https://pmc.ncbi.nlm.nih.gov/articles/PMC9592422/
[12] – https://europe.medtronic.com/xd-en/c/emea/spinal-orthopedic/kyphon-balloon-kyphoplasty.html
[13] – https://bmcsurg.biomedcentral.com/articles/10.1186/s12893-020-00753-4
[14] – https://www.mathurspinesurgery.com/imaging-in-kyphoplasty-for-spine-fractures/
[15] – https://ajronline.org/doi/10.2214/AJR.09.3647
[17] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3532655/
[21] – https://pmc.ncbi.nlm.nih.gov/articles/PMC11015514/
[22] – https://pubmed.ncbi.nlm.nih.gov/23142863/
[24] – https://pubmed.ncbi.nlm.nih.gov/16518574/
[25] – https://www.sciencedirect.com/science/article/pii/S1878875023014572
[26] – https://pmc.ncbi.nlm.nih.gov/articles/PMC2684146/
[27] – https://ejnpn.springeropen.com/articles/10.1186/s41983-023-00668-w
[29] – https://pubs.rsna.org/doi/abs/10.1148/radiol.2373041654
[30] – https://www.mdpi.com/2077-0383/14/9/2908
[31] – https://www.ajnr.org/content/39/5/798
[32] – https://pmc.ncbi.nlm.nih.gov/articles/PMC2248169/
[33] – https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/s12891-019-2807-6
[34] – https://ajronline.org/doi/10.2214/ajr.183.4.1831097
[35] – https://www.upmc.com/-/media/upmc/Services/neurosurgery/brain/documents/CompressionFractures.pdf
[36] – https://pmc.ncbi.nlm.nih.gov/articles/PMC9387994/
[37] – https://www.verywellhealth.com/kyphoplasty-recovery-5084121
[38] – https://www.neurosurgeryone.com/blog/addressing-concerns-about-pain-medications-after-spine-surgery/
[39] – https://www.bumrungrad.com/what-to-do-after-vertebroplasty-kyphoplasty
[41] – https://www.covenanthealth.com/wp-content/uploads/2023/06/Kyphoplasty.pdf
[43] –https://www.hss.edu/health-library/conditions-and-treatments/patient-guide-opioid-tapering